
 Definition
Definition
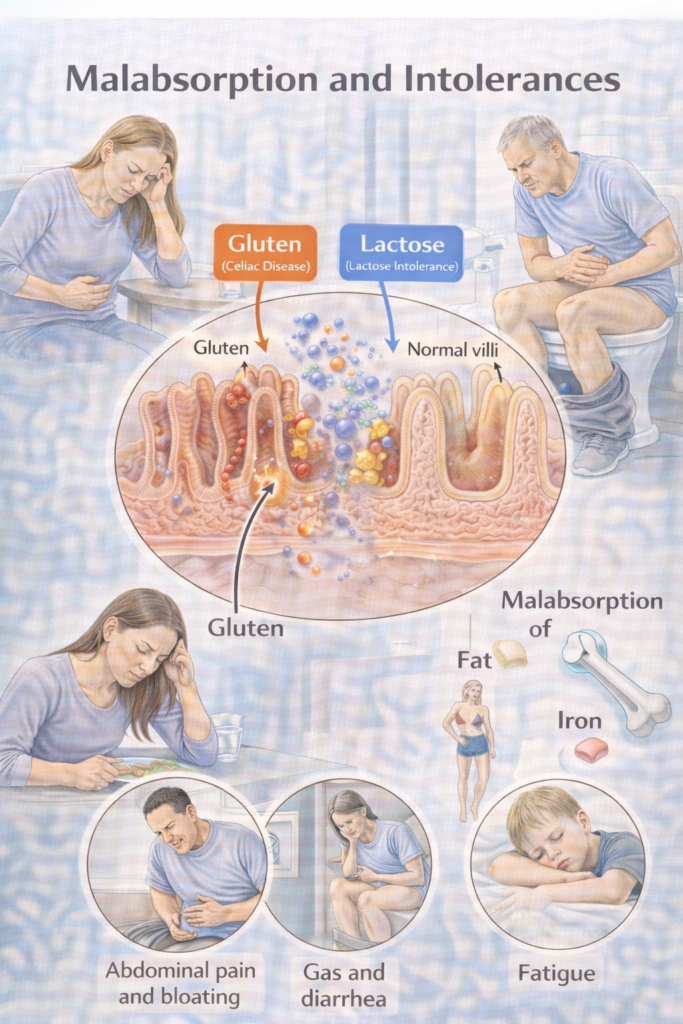
Malabsorption = impaired digestion and/or absorption of nutrients → diarrhoea (often steatorrhoea), weight loss, and micronutrient deficiencies.
Mechanistic buckets:
Intraluminal failure: inadequate digestive factors (e.g., pancreatic exocrine insufficiency [PEI], bile acid deficiency).
Mucosal failure: damaged absorptive surface (e.g., coeliac disease, Crohn’s).
Transport failure: impaired lymphatic transport (e.g., lymphangiectasia, short bowel).
 Clinical Features
Clinical Features
GI: Chronic diarrhoea (steatorrhoea = pale, greasy, difficult to flush), bloating, flatulence, abdominal discomfort.
Systemic: Weight loss, fatigue, micronutrient deficiencies (IDA, B12, folate, Vit D, Vit K).
Children: Faltering growth, delayed puberty.
Signs of deficiencies:
Iron/folate/B12 → anaemia, glossitis, neuropathy.
Vit D/Ca²⁺ → osteopenia, fractures.
Vit K → bruising, coagulopathy.
 High-Yield Hook:
High-Yield Hook:
Top 3 causes of steatorrhoea = Coeliac, PEI, BAD.
 Red flags (When to Refer) — Table
Red flags (When to Refer) — Table
| Tier | Key triggers (examples) | Action |
|---|---|---|
 Immediate emergency Immediate emergency | Severe dehydration, shock, peritonism, GI bleed | Same-day ED/acute take |
 Urgent gastroenterology Urgent gastroenterology | 🧠 Memory Box — NG12 CRC Referral (The “4-5-6 + Mass/FIT Rule”)
| Urgent clinic; follow NG12 cancer pathways and local imaging/colonoscopy protocols |
 Routine Routine | Positive coeliac serology; chronic diarrhoea not responding to first steps; suspected BAD/PEI/SIBO without instability | Specialist pathway for confirmatory tests and targeted therapy Gut |
💡Use FIT (faecal immunochemical test) where CRC risk is suspected per NICE NG12/DG56; do not delay urgent referral if clinical concern is high.
 Management
Management
1) General rule: Correct deficits + treat the driver + dietitian input. (all patients)
-
-
-
Correct fluid/electrolyte & micronutrient deficits.
-
Dietitian support early.
-
Refeeding risk: replace K⁺, Mg²⁺, PO₄³⁻ if severe malnutrition.
-
-
2) Cause-specific ladders
| Cause | First-line | Escalation / Notes |
|---|---|---|
| Coeliac disease | Lifelong GFD with specialist dietitian | Correct deficiencies (iron, folate, B12, Vit D, Ca²⁺). Adults need biopsy confirmation. Monitor tTG-IgA for adherence. |
| PEI (pancreatic exocrine insufficiency) | PERT (pancreatin/CREON with all meals/snacks), ADEK vitamins | Optimise dose (lipase units per g fat). Address alcohol/smoking. Nutrition support if severe. |
| Bile-acid diarrhoea (BAD) | Bile acid sequestrant (cholestyramine, colesevelam) titrated to stool control | Consider fat-soluble vitamin monitoring. Often chronic Rx. |
| SIBO | Empirical antibiotics (rifaximin, metronidazole; local protocol) | Identify/treat driver (motility disorder, strictures). May need cyclical therapy in recurrent cases. |
| Lactose intolerance / carbohydrate intolerance | Dietary exclusion to tolerance, then structured re-challenge | Lactase enzyme before dairy may help. Maintain Ca²⁺/Vit D intake. Distinguish from cow’s milk protein allergy. |
| Other (Giardia, short bowel, orlistat) | Targeted therapy (e.g., metronidazole for giardia, nutrition support for short bowel) | Stop culprit drug (e.g., orlistat). Specialist nutrition team for severe short bowel |