
 Definition
Definition
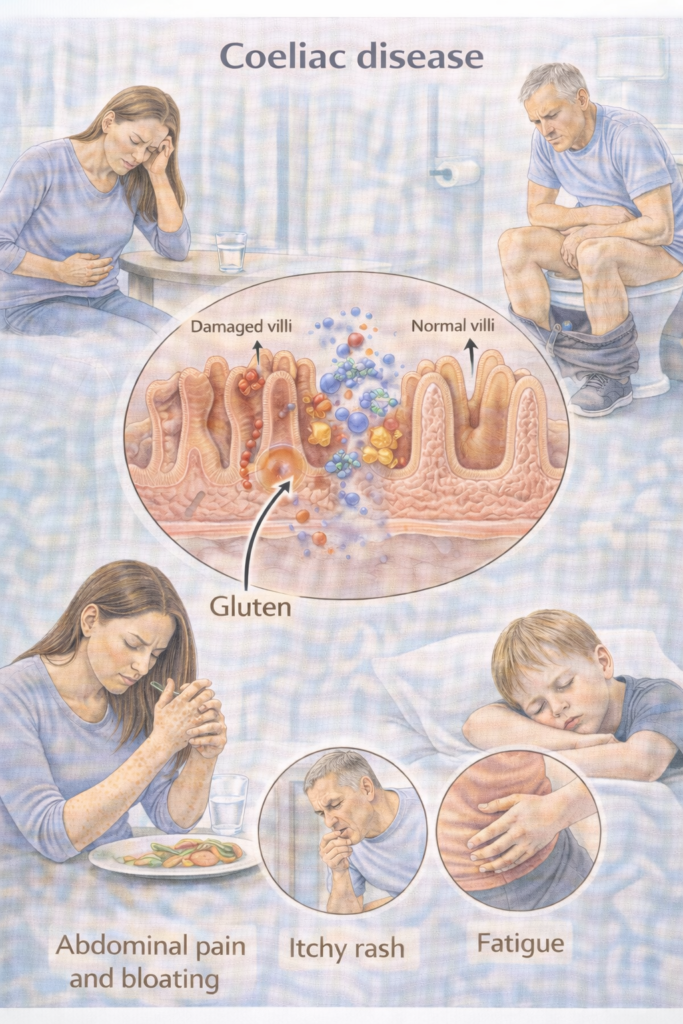
Coeliac disease is an autoimmune, gluten-driven enteropathy causing small-bowel mucosal damage and malabsorption in genetically susceptible people (HLA-DQ2/DQ8 haplotypes). Lifelong GFD (gluten-free diet) is the treatment.
 Pathophysiology
Pathophysiology
| Step | Pathophysiology | Exam clue |
|---|---|---|
 Gluten peptides Gluten peptides | Gliadin fragments reach lamina propria | Trigger antigen |
 tTG deamidation tTG deamidation | Increases HLA-DQ2/8 binding | Anti-tTG antibodies |
 T-cell activation T-cell activation | IFN-γ release, inflammation | Villous atrophy |
 B-cell activation B-cell activation | Anti-tTG, EMA, DGP antibodies | Used for serology |
 Mucosal damage Mucosal damage | Villous atrophy, crypt hyperplasia | Malabsorption (iron, folate, Ca, Vit D) |
 Mnemonic — “4A’s in Coeliac”
Mnemonic — “4A’s in Coeliac”
Autoimmunity (anti-tTG, EMA, DGP antibodies)
Atrophy (villous atrophy, crypt hyperplasia)
Absorption loss (malabsorption: diarrhoea, steatorrhoea, anaemia)
Associated risk (Enteropathy-associated T-cell lymphoma (EATL), adenocarcinoma, osteoporosis, other autoimmune conditions like T1DM, thyroid disease)
 Clinical Features
Clinical Features
-
GI: chronic/intermittent diarrhoea, bloating, abdominal pain, steatorrhoea, constipation (sometimes).
-
Systemic: iron/folate/B12 deficiency, weight loss, fatigue, osteopenia/osteoporosis.
-
Dermatology: DH (intensely itchy vesicular rash—elbows/knees/buttocks).
-
Children: faltering growth, delayed puberty, irritability.
 When to Test / Refer (NICE NG20)
When to Test / Refer (NICE NG20)
Who to test (serology): people with persistent GI symptoms or risk groups: IDA (iron-deficiency anaemia), weight loss, severe mouth ulcers, fatigue, type 1 diabetes at diagnosis, autoimmune thyroid disease, adults meeting IBS criteria, first-degree relatives, children with faltering growth. Test while eating gluten.
Referral pathway (adults & YP):
Positive serology → refer to GI for endoscopic duodenal biopsy to confirm/exclude coeliac disease. (NICE does not endorse adult “no-biopsy” diagnosis.)
Suspected DH → dermatology for skin biopsy with granular IgA + coeliac work-up.
 Management — Stepwise Ladder
Management — Stepwise Ladder
Before testing
Do not start a GFD. Take coeliac serology while eating gluten. Safety-net re: worsening symptoms/weight loss.
Confirm diagnosis
Adults: OGD (oesophagogastroduodenoscopy) with duodenal biopsies (per NG20). Children: follow ESPGHAN no-biopsy criteria where eligible (specialist).
Treatment initiation
Lifelong GFD with specialist dietitian input (label reading, cross-contamination, eating out, school/work).
Treat deficiencies (iron/B12/folate/vitamin D/calcium). Dental and fracture risk counselling.
Vaccination & general health
Consider pneumococcal vaccination if hyposplenism suspected; ensure routine immunisations up to date.
Lifestyle: weight/fitness; manage osteoporosis risk. (Bone health below.)
Assess non-response (NRCD)
Check hidden gluten, diet adherence (dietetic review), IBD, microscopic colitis, SIBO, pancreatic insufficiency, lactose intolerance; coeliac serology trend. Specialist referral for refractory coeliac disease.
 Prescribing notes
Prescribing notes
Gluten-free staple foods on NHS prescription are restricted by locality (often bread/flour only). Advise on supermarket options and Coeliac UK resources.
 Last updated in line with
Last updated in line with
NICE NG20 (Coeliac disease: recognition, assessment and management) — Published 2 Sep 2015, current online content; 2019 surveillance retained biopsy-based diagnosis in adults. NICE+1
NICE QS134 (Coeliac disease – Quality Standard) — Biopsy within 6 weeks of referral. NICE
ESPGHAN 2020 (Paediatric no-biopsy pathway). ESPGHAN
BSG (British Society of Gastroenterology) adult guideline — current page notes under review for 2025; use alongside NICE. British Society of Gastroenterology
NHS England (Gluten-free foods prescribing policy) — local restriction of items (commonly bread/flour). NHS England
- PARA-aligned, reviewed February 2026