
 Definition
Definition
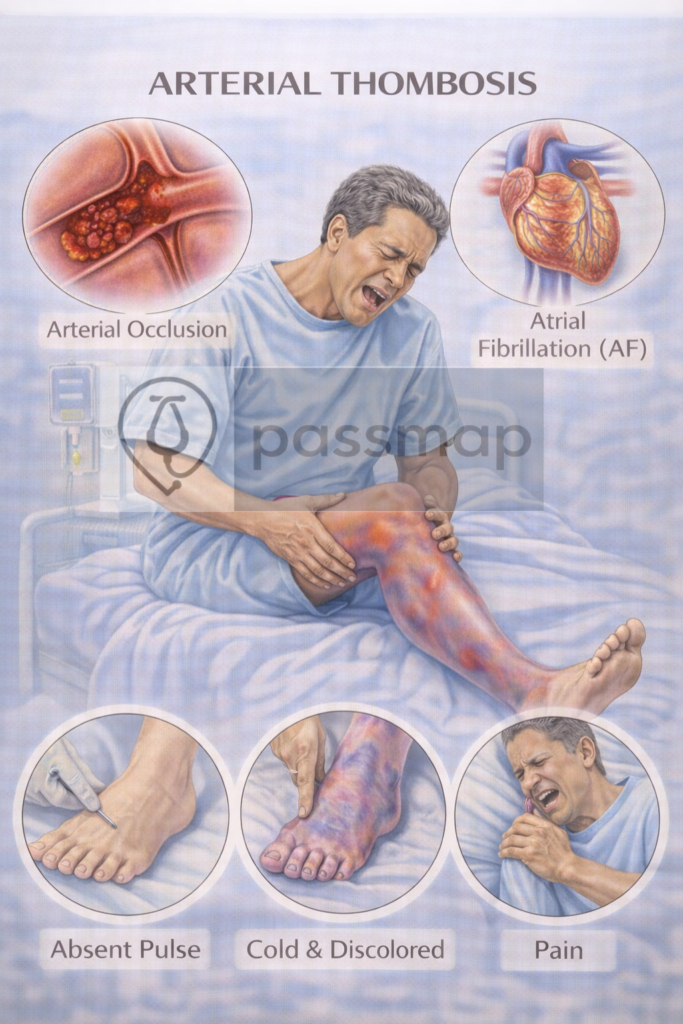
Arterial thrombosis is the formation of a blood clot in an artery, causing partial or complete obstruction of blood flow. It commonly leads to life-threatening events such as:
Myocardial infarction (MI) – Coronary artery thrombosis
Ischaemic stroke – Cerebral artery thrombosis
Acute limb ischaemia – Peripheral artery thrombosis
Pathophysiology
Arterial clots form primarily due to ruptured atherosclerotic plaques in high-flow vessels, leading to platelet-rich (“white”) thrombi.
Virchow’s triad in arterial thrombosis:
- Thrombosis (In-situ): Clot forms directly on a ruptured atherosclerotic plaque.
- Embolism (Traveling): Clot originates elsewhere (e.g., Atrial Fibrillation) and occludes a distal vessel.
- The “White Clot”: Driven by platelet aggregation; therefore, antiplatelets are the cornerstone of long-term management.
Risk Factors
 Mnemonic: ATHEROMA
Mnemonic: ATHEROMA
Ageing
Tobacco use
Hypertension
Elevated lipids
Renal dysfunction
Obesity
Male sex
Atrial fibrillation (embolic risk)
 EXAM ANCHOR – ACUTE LIMB ISCHAEMIA
EXAM ANCHOR – ACUTE LIMB ISCHAEMIA
PARA focuses heavily on the 6 P’s and the urgency of surgical referral.
The 6 P’s: Pain, Pallor, Pulselessness, Paraesthesia, Paralysis, Perishingly cold.
Threatened Limb: Paraesthesia and Paralysis are late signs indicating the limb is at risk of permanent necrosis.
Immediate Step: IV Unfractionated Heparin (UFH) bolus + Urgent Vascular Review.
Note: UFH is preferred over LMWH because it is quickly reversible with Protamine if emergency surgery is required.
📌 PARA commonly asks:
“A patient with AF has a cold, pulseless leg. What is the most appropriate immediate pharmacological step?”
Management
 Mnemonic: ACT FAST
Mnemonic: ACT FAST
Aspirin (antiplatelet)
Clopidogrel or dual antiplatelet therapy (DAPT)
Long-term: Switch to Clopidogrel 75mg daily.
The Trap: Do not start Clopidogrel immediately in the acute phase; Aspirin is the priority for the first two weeks.
Thrombolysis (e.g. alteplase) – for stroke if within time window
Fibrinolysis (in STEMI or major embolism, if PCI not available)
Angioplasty / PCI or stenting (urgent)
Statin initiation
Treat underlying cause (e.g. hypertension, diabetes)
EXAM ANCHOR – ACUTE LIMB ISCHAEMIA
PARA focuses on the “Urgent Referral” aspect.
Investigation: Handheld Doppler (if pulses not palpable). If Doppler signals are absent, it is a surgical emergency.
Immediate Management: IV Unfractionated Heparin (to prevent clot propagation).
Analgesia and IV fluids.
Urgent Vascular Review for reperfusion (Embolectomy vs. Bypass).
📌 PARA commonly asks:
“A patient has a cold, pulseless leg with loss of sensation. What is the most appropriate immediate pharmacological step?”