
 Definition
Definition
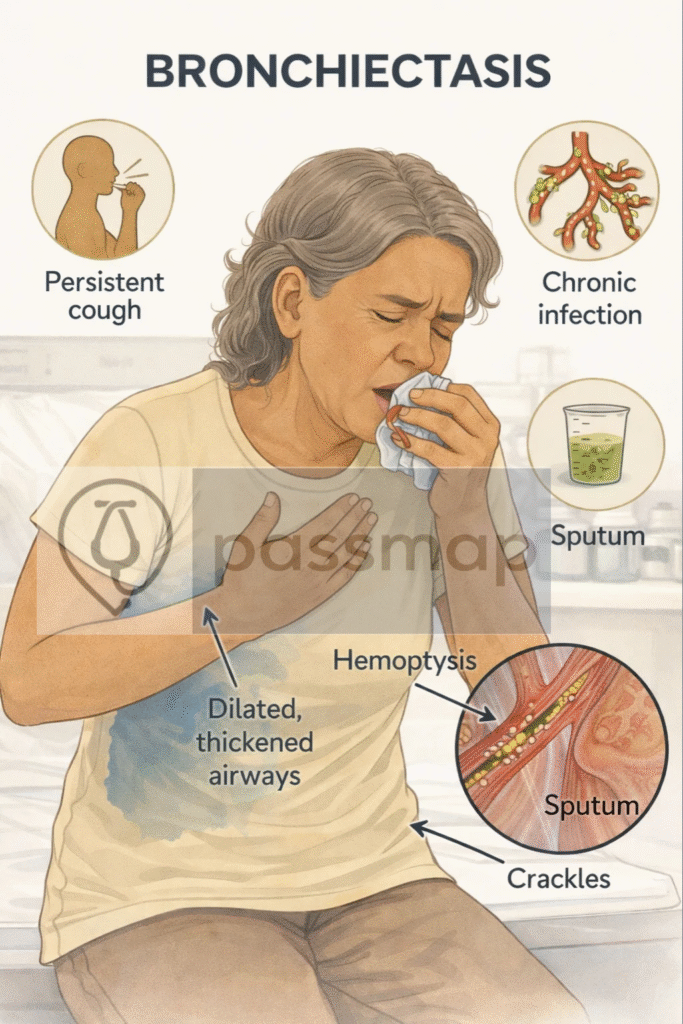
Bronchiectasis is an irreversible abnormal dilatation of the bronchi due to chronic infection and inflammation, resulting in impaired mucus clearance and persistent cough with sputum production.
 Pathophysiology
Pathophysiology
 Mnemonic: CYCLE
Mnemonic: CYCLE
Chronic infection →
Yielding inflammation
Ciliary damage
Loss of airway tone
Expansion of bronchi (permanent dilatation)
→ Leads to mucus stasis, colonisation, and recurrent infections.
 Clinical Features
Clinical Features
Mnemonic: COUGH SPIT
-
Chronic productive cough
-
Overproduction of sputum (purulent, foul-smelling)
-
Up to 2+ exacerbations per year
-
Green/yellow mucus plugs
-
Haemoptysis (mild to massive)
-
Shortness of breath
-
Pleuritic chest pain
-
Infections recurrent
-
Tiredness (systemic symptoms)
 EXAM ANCHOR 3 – DIAGNOSIS (GOLD STANDARD)
EXAM ANCHOR 3 – DIAGNOSIS (GOLD STANDARD)
High-resolution CT (HRCT) = diagnostic gold standard
Key CT signs:
Tram-track sign
Signet-ring sign
Cystic bronchial dilatation
CXR may be normal and does not exclude bronchiectasis
 PARA commonly asks:
PARA commonly asks:
Which investigation confirms bronchiectasis?
EXAM ANCHOR 4 – FIRST-LINE MANAGEMENT LONG TERM MANAGEMENT
First-line management includes Active Cycle of Breathing Techniques (ACBT) and checking/supplementing Vitamin D levels.
Antibiotics alone are not sufficient long-term management
Vaccinations + smoking cessation are mandatory supportive care
PARA commonly asks:
Most important long-term management strategy in bronchiectasis?
 Answer: Airway clearance physiotherapy
Answer: Airway clearance physiotherapy
EXAM ANCHOR 5 – EXACERBATIONS
Always send sputum culture before antibiotics
Treat exacerbations with 14-day antibiotics
If Pseudomonas aeruginosa is isolated for the first-time, NICE recommends eradication therapy (specialist-led) rather than standard symptom management.
PARA commonly asks:
Best next step in an acute exacerbation?
EXAM ANCHOR 6 – FREQUENT EXACERBATORS
≥3 exacerbations/year → consider long-term macrolide
Before starting long-term macrolides (Azithromycin), you must perform:
Sputum culture for NTM (Non-Tuberculous Mycobacteria) to prevent resistance.
Baseline ECG to check the QTc interval (Macrolides can prolong QTc).
Chronic Pseudomonas colonisation → inhaled antibiotics
Specialist supervision required
PARA commonly asks:
Indication for long-term antibiotics in bronchiectasis?
🧐Differentials
Mnemonic: CHAPS
-
COPD
-
Haemoptysis from TB/lung cancer
-
Asthma
-
Pneumonia
-
Sinusitis/post-nasal drip
 Key PARA Exam Traps
Key PARA Exam Traps
 HRCT is gold standard → tram-track sign, ring shadows
HRCT is gold standard → tram-track sign, ring shadows
Always send sputum culture, especially in exacerbations
Cough + sputum + coarse crackles = high yield
Daily chest physio is first-line long term management
Long-term abx for frequent exacerbators