
 Definition
Definition
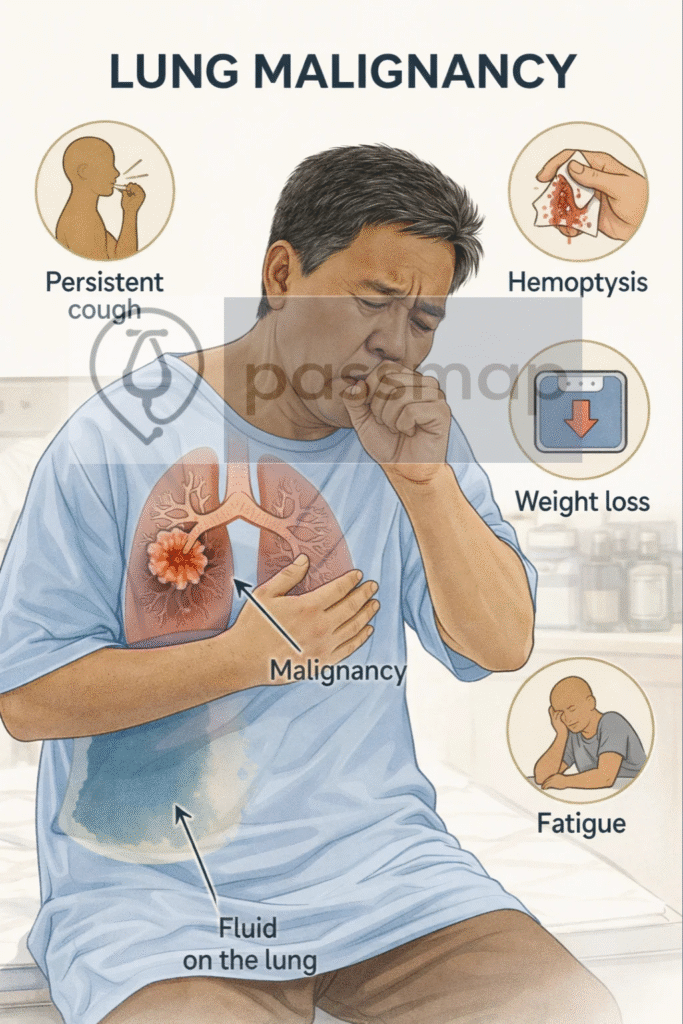
Lung Malignancy is a malignant tumour originating in the lung tissue. It is the leading cause of cancer-related death in the UK.
 Clinical Features
Clinical Features
🧠 Mnemonic: SPHERE
Symptoms: cough (persistent/new/change), dyspnoea
Pain: chest pain
Haemoptysis
Effusion (pleural)
Recurring infections (e.g. pneumonia)
Energy low (weight loss, fatigue)
🧠 Late signs: hoarseness (recurrent laryngeal nerve), SVC obstruction, clubbing, Horner’s syndrome, bone pain, seizures (mets)