
 Clinical Features
Clinical Features
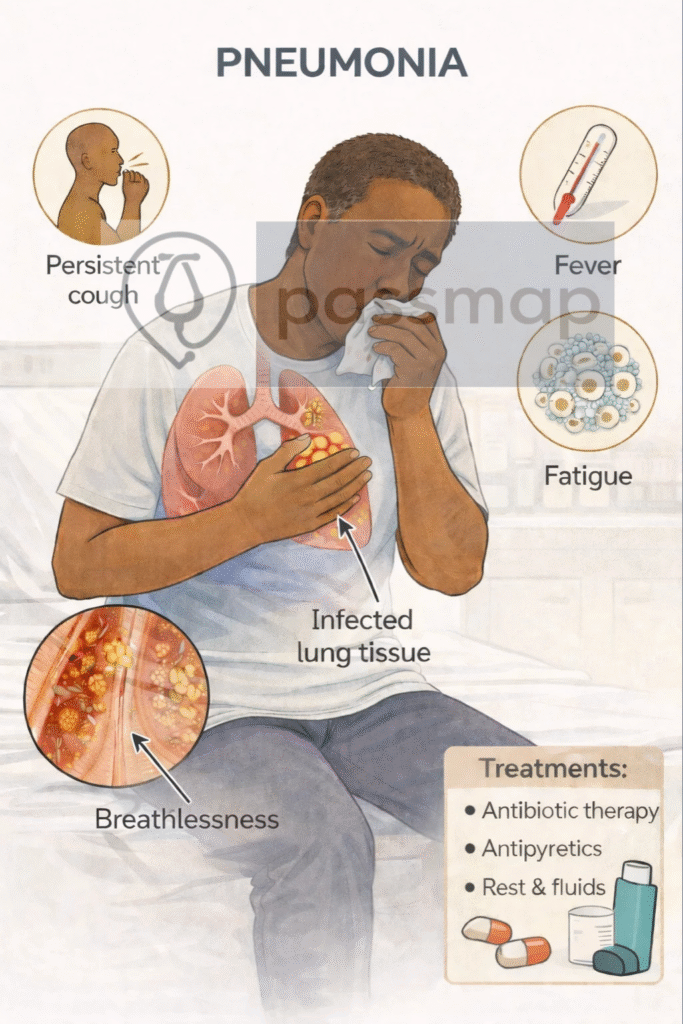
Mnemonic: COPS
Cough (productive ± blood-streaked)
Over 38°C fever
Pleuritic chest pain
Shortness of breath
Others: rigors, confusion (elderly), fatigue
 EXAM ANCHOR – DIAGNOSIS
EXAM ANCHOR – DIAGNOSIS
Chest X-ray confirms pneumonia
Clinical features alone are insufficient
Normal early CXR does not exclude pneumonia
 PARA commonly asks:
PARA commonly asks:
A patient presents with fever, cough, and pleuritic chest pain. Which investigation is required to confirm the diagnosis of pneumonia?