
 Definition
Definition
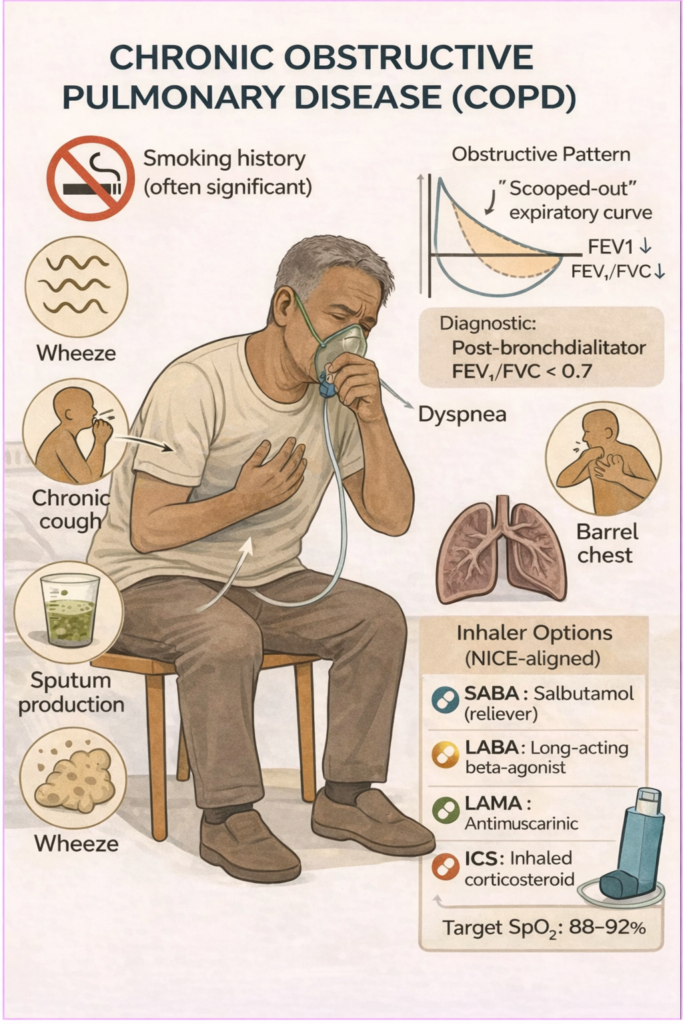
Persistent airflow obstruction that is not fully reversible due to chronic inflammation from smoking or environmental exposure.
Includes:
Chronic bronchitis: productive cough ≥3 months for ≥2 consecutive years
Emphysema: alveolar wall destruction & airspace enlargement
 Pathophysiology
Pathophysiology
Inhaled irritants (e.g. smoke) → inflammation → mucus hypersecretion + alveolar destruction
Leads to air trapping, reduced gas exchange, and increased work of breathing
 Risk Factors
Risk Factors
Mnemonic: SCARE
Smoking (most important)
Cooking fuel/air pollution (biomass exposure)
Alpha-1 antitrypsin deficiency
Repeated childhood infections
Environmental/occupational exposure (e.g. coal, dust)
 Clinical Features
Clinical Features
Mnemonic: COUGHED
Chronic productive cough
Overexertion causes dyspnoea
Unusual wheeze
Gradual onset of symptoms
Hyperinflated chest
Exercise limitation
Daily sputum production
 EXAM ANCHOR – BRONCHODILATORS (PARA)
EXAM ANCHOR – BRONCHODILATORS (PARA)
 PARA commonly asks:
PARA commonly asks:
What is the first-line bronchodilator regimen in an acute COPD exacerbation?
 Answer: Short-acting β₂-agonist or short-acting muscarinic antagonist (salbutamol or ipratropium)
Answer: Short-acting β₂-agonist or short-acting muscarinic antagonist (salbutamol or ipratropium)
 Complications
Complications
Mnemonic: CHAP
Cor pulmonale (right heart failure)
Hypercapnic respiratory failure
Acute exacerbations
Pneumothorax (esp. in bullous disease)
 Key PARA Exam Traps – COPD
Key PARA Exam Traps – COPD
 Post-bronchodilator FEV₁/FVC < 0.7 confirms COPD
Post-bronchodilator FEV₁/FVC < 0.7 confirms COPD
Irreversible airflow obstruction (reversible = asthma)
Smoking cessation is the only disease-modifying intervention
ICS not first-line → use only when there are:
• Frequent exacerbations (≥2/year or ≥1 hospital admission) despite bronchodilators, or
• Steroid responsiveness (e.g. asthma history or blood eosinophils ≥300 cells/µL)
Exacerbation O₂ target 88–92% (avoid over-oxygenation)
LTOT only if PaO₂ ≤ 7.3 kPa (stable COPD)
Treatment escalation guided by MRC + exacerbations, not FEV₁ alone
Chronic hypoxia → polycythaemia, cor pulmonale
Sudden deterioration → consider pneumothorax (bullae)