
Investigations
 First-Line
First-Line
ABPI (Ankle-Brachial Pressure Index):
<0.9 = diagnostic of PAD
<0.5 = severe disease
Duplex Doppler Ultrasound – assess blood flow and stenosis
 EXAM ANCHOR 1 – THE ABPI INTERPRETATION
EXAM ANCHOR 1 – THE ABPI INTERPRETATION
The Ankle-Brachial Pressure Index (ABPI) is your first-line diagnostic test.
Normal: 1.0 – 1.2
PAD: < 0.9
Critical Limb Ischaemia: < 0.5 (or ankle pressure < 50 mmHg)
PARA TRAP – The Calcified Vessel: In patients with Diabetes or CKD, arteries can become calcified and non-compressible. This leads to a falsely high ABPI (> 1.2). If you see a high ABPI in a symptomatic diabetic, the next step is a Toe-Brachial Pressure Index (TBPI) or Duplex Ultrasound.
 Second-Line
Second-Line
MR Angiography or CT Angiography – pre-intervention planning
Bloods: FBC, U&Es, HbA1c, Lipids, LFTs, ESR/CRP
ECG – evaluate cardiovascular risk
 Clinical Features –
Clinical Features –
Mnemonic: 6 Ps (acute) and CLAUDICATE (chronic)
Acute Limb Ischaemia – 6 Ps:
Pain
Pallor
Pulselessness
Paralysis
Paraesthesia
Perishing cold
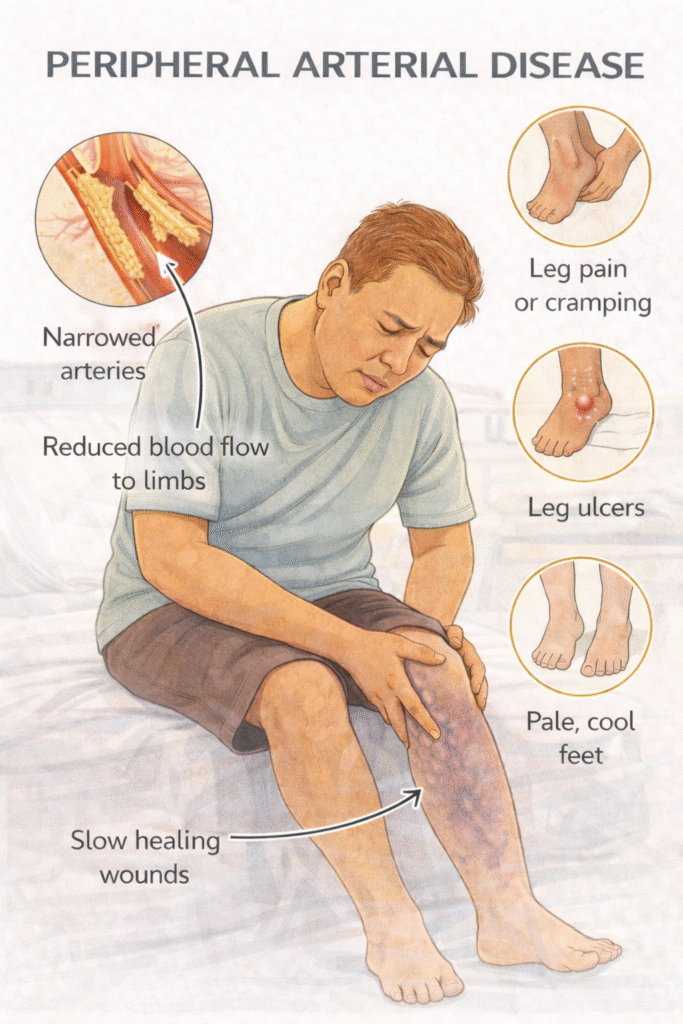
Chronic PAD – Mnemonic: CLAUDICATE
Cramping calf pain
Loss of hair
Abnormal pulses
Ulcers (arterial)
Dry, shiny skin
Intermittent claudication
Cool peripheries
ABPI <0.9
Toe pallor
Erectile dysfunction (Leriche syndrome)
EXAM ANCHOR 1 – CHRONIC VS. ACUTE FEATURES
Intermittent Claudication: Pain is reproducible (occurs at the same distance every time) and relieved by rest.
Critical Limb Ischaemia (CLI): Defined by the “Triad of Trouble”:
Rest Pain: Burning pain at night, relieved by hanging the leg over the edge of the bed (gravity helps perfusion).
Ulceration: Typically “punched out” ulcers on the toes or heels.
Gangrene.
EXAM ANCHOR 1 – MANAGEMENT (NICE CG147)
The PARA tests your ability to prioritize medical management before jumping to surgery.
- Antiplatelet: Clopidogrel 75mg is the first-line choice (Aspirin is second-line for PAD).
- Statin: Atorvastatin 80mg (High-intensity) for all patients.
- Supervised Exercise Programme: This is the first-line non-drug treatment for intermittent claudication. Patients should walk until the pain is near-maximal, then rest, then repeat for 30–45 mins, 3x per week.
- Naftidrofuryl oxalate: If exercise and risk factor modification fail, this can be offered for symptom relief (NICE alternative to Cilostazol).