
 Definition
Definition
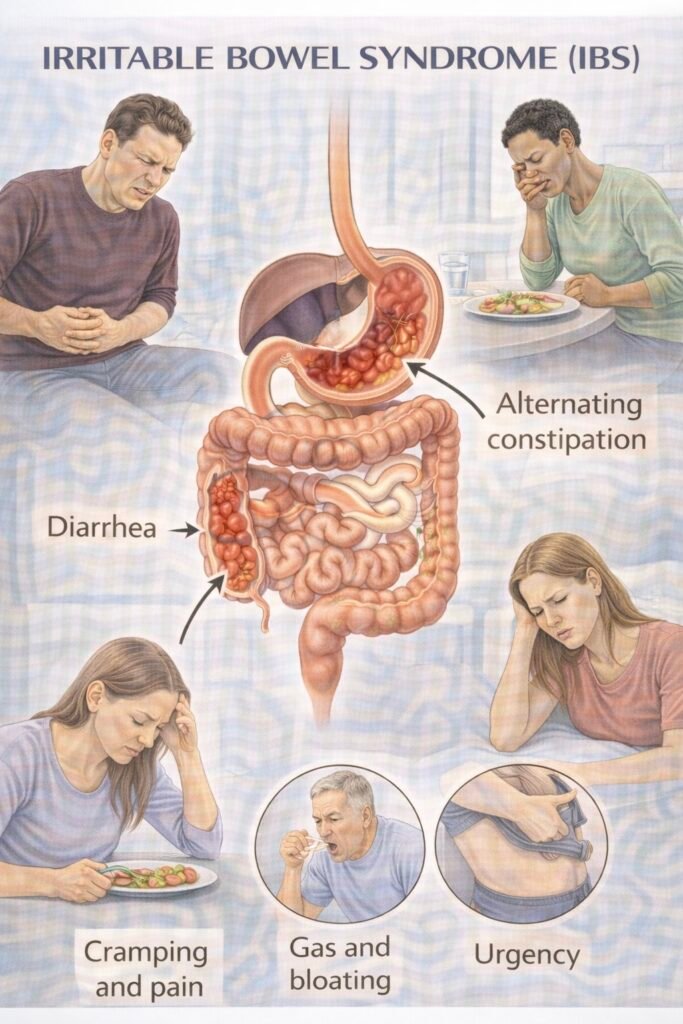
IBS (Irritable Bowel Syndrome) is a functional bowel disorder causing recurrent abdominal pain with altered bowel habit.
IBD Subtypes:
- IBS-C constipation-predominant
- IBS-D diarrhoea-predominant /
- IBS-M mixed
- IBS-U unclassified without structural disease.
- Use a positive diagnosis approach (Rome IV criteria)
 Clinical features
Clinical features
-
Crampy lower abdominal pain linked to bowel movements
-
Bloating/distension (often post-prandial)
-
Altered habit by subtype:
-
IBS-D: loose stools, urgency, “morning rush”
-
IBS-C: hard stools, straining, incomplete emptying
-
IBS-M: swings hard ↔ loose
-
-
Mucus can occur; nocturnal symptoms uncommon (if waking up from sleep → think organic)
Investigations (to support a positive diagnosis)
| Test | Why / When | How / Notes |
|---|---|---|
| FBC (full blood count) | Screen anaemia/red flags | IDA → consider NG12/2WW pathway rather than IBS |
| CRP / ESR (C-reactive protein / erythrocyte sedimentation rate) | Functional vs inflammatory | Normal supports IBS; raised → IBD/infection |
| Coeliac serology – tTG-IgA + total IgA (tissue transglutaminase IgA) | Exclude coeliac disease | If IgA deficient, use an IgG-based test |
| Faecal calprotectin | Adults with recent-onset lower-GI symptoms when cancer not suspected (IBD vs IBS) | Not needed in classic long-standing IBS without red flags |
| FIT (faecal immunochemical test) | If CRC concern | Refer if FIT ≥10 µg Hb/g; don’t delay if high suspicion |
| TSH (thyroid-stimulating hormone) / serum calcium | If clinically indicated | Not routine for every patient |
| Targeted stool tests | Travel/infectious risk | Use selectively |
Supportive tools: 2-week symptom & stool diary; subtype using the Bristol Stool Form Scale (BSFS):
 BSFS = Bristol Stool Form Scale
BSFS = Bristol Stool Form Scale
Types 1–2 = hard, 3–5 = normal, 6–7 = loose/watery.
 Management — (adults, primary care first)
Management — (adults, primary care first)
 Foundations
Foundations
Positive diagnosis; explain brain–gut axis. Regular meals; fluids; activity; limit caffeine/alcohol/fizzy drinks; fruit ≤3/day; start 2-week diary.
 Diet (first-line)
Diet (first-line)
Soluble fibre (psyllium/ispaghula). Avoid insoluble bran if worse; reduce resistant starch.
 Targeted symptom relief
Targeted symptom relief
-
Pain/bloat: antispasmodic (mebeverine/hyoscine) or peppermint oil.
-
IBS-D: loperamide PRN/titrate.
-
IBS-C: PEG (polyethylene glycol/macrogol); avoid lactulose if bloating.
 Second-line
Second-line
Low-FODMAP diet (4–6 weeks) with a dietitian, then re-introductions.
Low-dose TCA (e.g., amitriptyline 10 mg nocte; titrate; review at 4–6 weeks). Consider SSRI (selective serotonin reuptake inhibitor) if TCA not tolerated or mood/anxiety dominates.
 Third-line / Specialist
Third-line / Specialist
Linaclotide for refractory IBS-C (specialist-initiated per local pathway).
Gut-directed CBT/psychological therapies.
Assess for BAD, microscopic colitis, or pelvic floor dysfunction if refractory.