
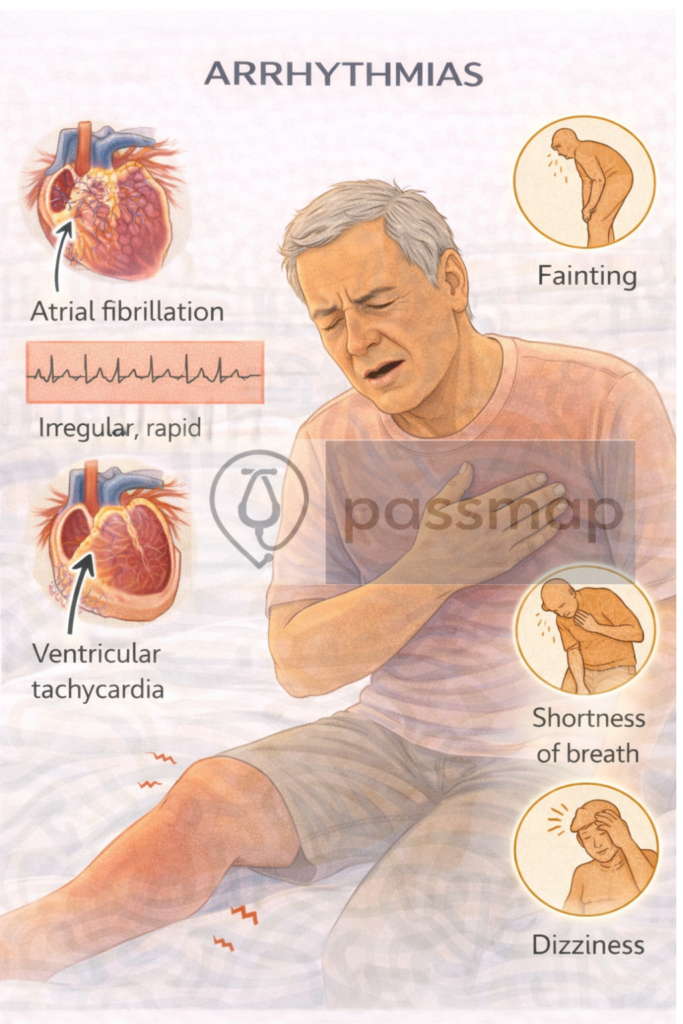
⚡️ Supraventricular Arrhythmias
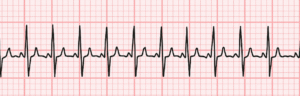
Atrial Fibrillation (AF)

Most common sustained arrhythmia
Irregularly irregular rhythm, no P waves
Risk of stroke: use CHA₂DS₂-VASc score
Anticoagulation if ≥2 (men) or ≥3 (women)
🧠 Mnemonic: ABC for AF
Anticoagulate
Beta-blocker or rate control
Cardioversion (electrical or pharmacological)
Rate vs Rhythm Control:
Rate: 1st line for most (BB, CCB, digoxin)
Rhythm: Younger, symptomatic, 1st episode (flecainide, amiodarone, cardioversion)
Atrial Flutter

Similar management to AF
Sawtooth ECG pattern
More amenable to ablation
SVT (AVNRT/AVRT)
Sudden onset palpitations, regular narrow complex tachycardia
Management:
Vagal manoeuvres (1st line)
Adenosine IV (2nd line) – brief asystole
Long-term: BB, CCB, ablation
Bradyarrhythmias
Sinus Bradycardia

Often benign (athletes, sleep)
Treat if
symptomatic (e.g. dizziness, syncope)
Heart Block

| Type | ECG Features | Notes |
|---|---|---|
| 1st degree | PR >200 ms | Usually benign |
| 2nd degree I | Progressive PR prolongation → dropped beat | Mobitz I (Wenckebach) |
| 2nd degree II | Dropped beat with constant PR | Mobitz II → risk of asystole |
| 3rd degree | Complete dissociation (P ≠ QRS) | Requires pacing |
(ALS protocol)