
 Definition
Definition
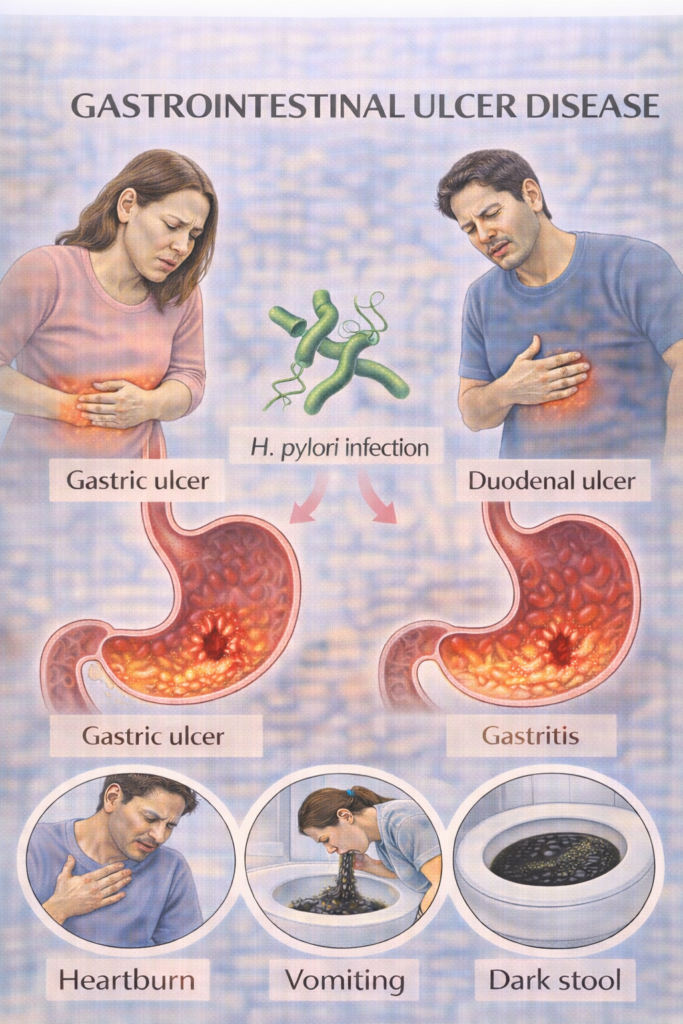
Mucosal ulceration in the stomach (gastric ulcer) or proximal duodenum (duodenal ulcer), due to imbalance between mucosal defences and acid/pepsin exposure.
 Clinical Features (Mnemonic: DUPE)
Clinical Features (Mnemonic: DUPE)
Dyspepsia:
Duodenal ulcer: pain relieved by food, worse at night
Gastric ulcer: pain worsened by food
Ulcer complications: bleeding, perforation, obstruction
Post-prandial fullness / bloating
Epigastric tenderness on palpation
 OGD Referral Criteria:
OGD Referral Criteria:
Refer for urgent endoscopy if:
1️⃣ Urgent – 2 Week Wait (ALARM55)
Anaemia (iron deficiency)
Loss of weight (unintentional)
Anorexia
Recent-onset progressive dysphagia
Melaena / haematemesis
55 – Age ≥55 with new-onset symptoms
2️⃣ Non-Urgent OGD – Without ALARM Features
Age ≥55 with unexplained, persistent dyspepsia
Persistent symptoms after 4–8 week PPI trial + negative H. pylori
Unexplained iron-deficiency anaemia without obvious source
 Differentiating Gastric vs Duodenal Ulcers
Differentiating Gastric vs Duodenal Ulcers
| Feature | Gastric Ulcer | Duodenal Ulcer |
|---|---|---|
| Pain | Worsened by food | Relieved by food |
| Risk of malignancy | Yes (requires biopsy) | Rare |
| Common in | Older adults | Younger patients |
| Location | Lesser curvature of stomach | First part of duodenum |