
 Definition
Definition
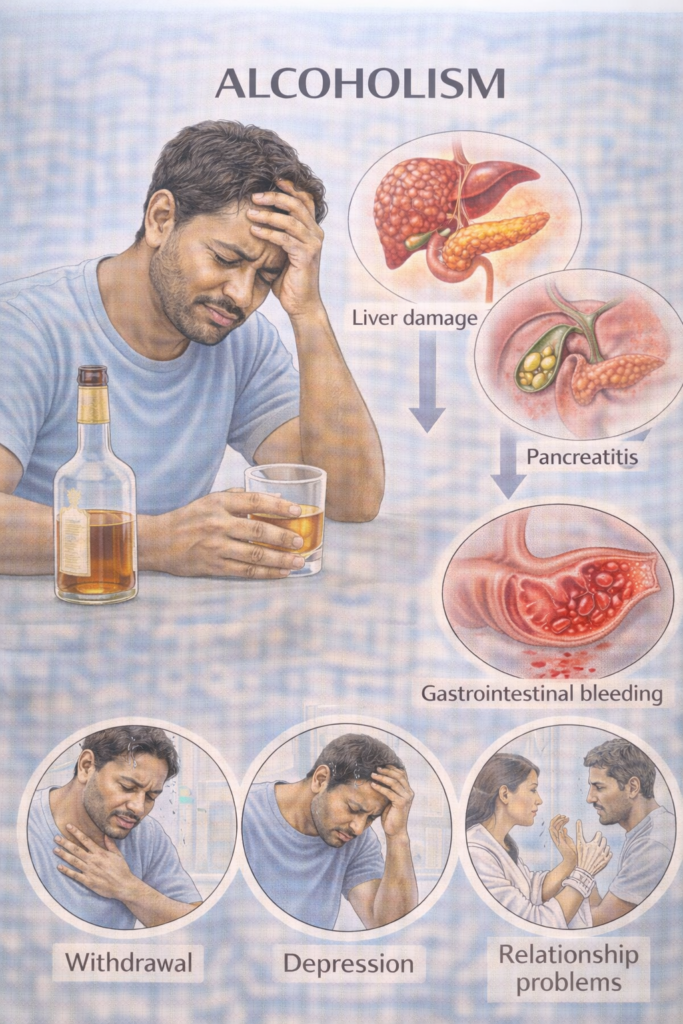
Chronic, harmful use of alcohol leading to physical, psychological, and social impairment. Strong association with liver disease, GI disorders, mental health conditions, and increased mortality.
 Risk Factors
Risk Factors
Family history (genetic predisposition).
Mental health: depression, anxiety, trauma, social isolation.
Social: unemployment, deprivation, peer culture.
Biological: male sex, early onset drinking.
 Epidemiology (UK)
Epidemiology (UK)
~25% of adults drink above recommended limits (ONS, 2023).
Higher prevalence in men (2× risk).
↑ Burden in Scotland & Northern England.
Ethnicity: ↑ risk in White British; lower in South Asian Muslim populations (religious abstinence).
Alcohol-related hospital admissions: >980,000/year in England.
🔬 Pathophysiology (simplified)
Ethanol → metabolised in liver (alcohol dehydrogenase → acetaldehyde → acetate).
Excess acetaldehyde → toxic to hepatocytes → oxidative stress, inflammation.
Steatosis → steatohepatitis → fibrosis → cirrhosis → HCC.
CNS effects: GABA agonism (sedation) + NMDA antagonism (withdrawal hyperexcitability).
Dependence: altered reward pathways (dopamine, glutamate).
 Guidelines referenced: NICE CG115 (Alcohol-use disorders), SIGN 74 (Management of harmful drinking), NICE NG50 (Cirrhosis).
Guidelines referenced: NICE CG115 (Alcohol-use disorders), SIGN 74 (Management of harmful drinking), NICE NG50 (Cirrhosis). PASSMAP ensures all content is PARA-aligned, exam-focused, and NICE-compliant.
PASSMAP ensures all content is PARA-aligned, exam-focused, and NICE-compliant.
- PARA-aligned, reviewed February 2026