
 Definition
Definition
Acute or chronic inflammation of the pancreas due to premature activation of pancreatic enzymes, leading to autodigestion, inflammation, and systemic complications.
 Pathophysiology
Pathophysiology
-
Enzyme activation (trypsinogen → trypsin) → autodigestion.
-
Triggers: gallstones, alcohol, hypertriglyceridaemia, trauma, ERCP, drugs.
-
Can → necrosis, pseudocyst, systemic inflammatory response (SIRS).
 Causes (Mnemonic: I GET SMASHED)
Causes (Mnemonic: I GET SMASHED)
-
Idiopathic
-
Gallstones (most common UK)
-
Ethanol
-
Trauma
-
Steroids
-
Mumps / viral infections
-
Autoimmune
-
Scorpion sting (rare)
-
Hyperlipidaemia / Hypercalcaemia
-
ERCP (Endoscopic retrograde cholangiopancreatography)
-
Drugs (azathioprine, valproate, thiazides, tetracyclines)
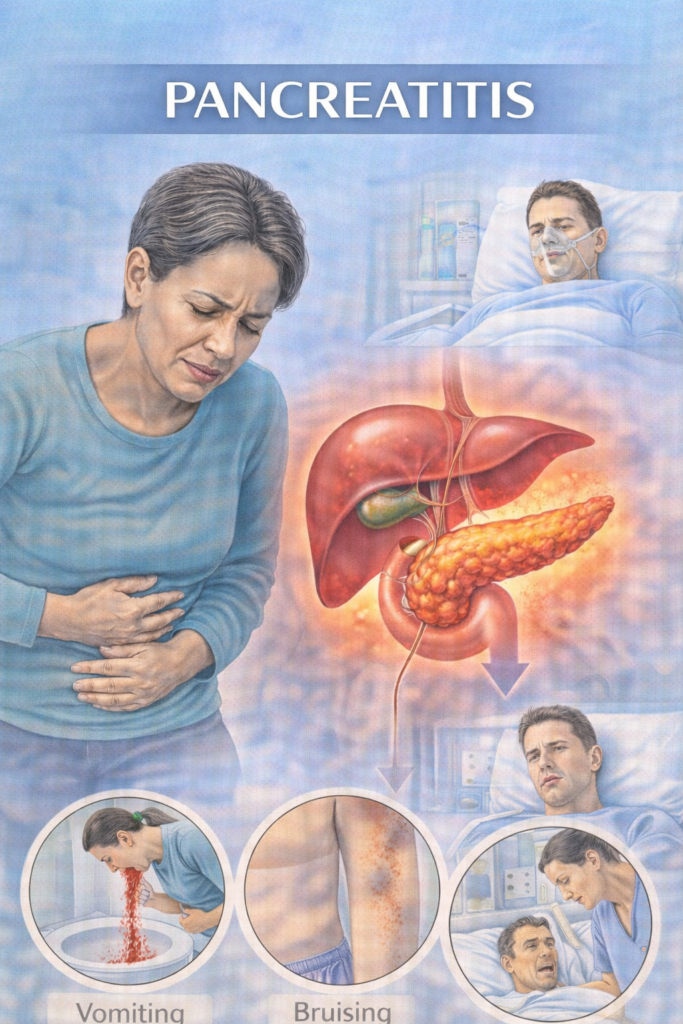
📋 Clinical Features
Severe epigastric pain radiating to back, relieved by sitting forward
Nausea, vomiting, anorexia
Abdominal tenderness ± guarding
Fever, tachycardia, hypotension
Severe: Grey-Turner’s sign (flank bruising), Cullen’s sign (periumbilical bruising)
 Glasgow Score (PANCREAS) – Assess within 48 hrs
Glasgow Score (PANCREAS) – Assess within 48 hrs
| Criterion | Cut-off | Score |
|---|---|---|
| PaO₂ | < 8 kPa (60 mmHg) | +1 |
| Age | > 55 years | +1 |
| Neutrophils (WCC) | > 15 × 10⁹/L | +1 |
| Calcium | < 2.0 mmol/L | +1 |
| Renal function (Urea) | > 16 mmol/L | +1 |
| Enzymes (LDH) | > 600 U/L | +1 |
| AST/ALT | > 200 U/L | +1 |
| SugarGlucose) | > 10 mmol/L | +1 |
 Interpretation:
Interpretation:
Score 0–2 → mild pancreatitis
Score ≥3 → severe pancreatitis (↑ risk of complications/mortality)