
 Definition
Definition
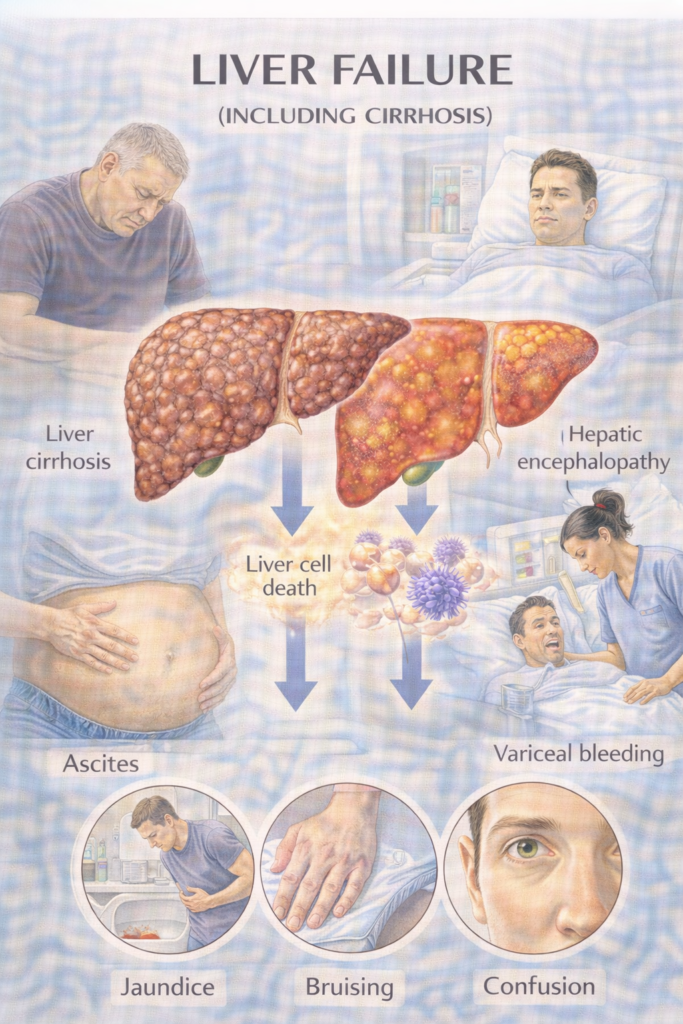
Liver failure = loss of hepatic synthetic & detoxifying capacity → coagulopathy (INR ≥1.5), jaundice, ± encephalopathy.
Cirrhosis = end-stage diffuse hepatic fibrosis with nodular remodelling & portal hypertension; can be compensated or decompensated (ascites, variceal bleeding, jaundice, encephalopathy).
Acute liver failure (ALF) = INR ≥1.5 + any encephalopathy, no prior cirrhosis.
Acute-on-chronic liver failure (ACLF) = acute decompensation of cirrhosis with organ failure(s) & high short-term mortality.
 Aetiology / Risk (by jaundice category)
Aetiology / Risk (by jaundice category)
| Category | Examples (high-yield) | PARA Exam Traps |
|---|---|---|
| Pre-hepatic (before liver – ↑ unconjugated bilirubin) | Haemolysis: autoimmune haemolysis, sickle cell, thalassaemia, G6PD deficiency. Gilbert’s syndrome (benign ↓UGT activity). | Normal LFTs, ↑ unconjugated bilirubin, no bilirubinuria. Gilbert’s often triggered by stress/fasting. |
| Hepatic (intra-liver – impaired conjugation/excretion) | Alcohol: chronic harmful use, binge → decompensation. Viral: HBV, HCV (chronic), HAV/HEV (acute; HEV high risk in pregnancy). Metabolic: MASLD, haemochromatosis, Wilson’s disease, α-1 antitrypsin deficiency. Autoimmune/cholestatic: AIH, PBC, PSC. Vascular/Ischaemic: Budd–Chiari, shock liver. Drugs/Toxins: Paracetamol, valproate, isoniazid, methotrexate, amiodarone, alcohol. Other: Malignancy infiltration, pregnancy syndromes (AFLP, HELLP). | Mixed pattern on LFTs: ↑ ALT/AST ± ↑ bilirubin. Severe cases → prolonged INR/low albumin. |
| Post-hepatic (obstructive/cholestatic – ↑ conjugated bilirubin) | Gallstones (choledocholithiasis). Malignancy: pancreatic, ampullary, cholangiocarcinoma. Strictures, PSC. Parasites (rare in UK). | Dark urine, pale stools, pruritus. LFTs: ↑ALP, ↑GGT > transaminases. Courvoisier’s law: palpable, non-tender GB = malignancy. |
 High-Yield Liver Disorders
High-Yield Liver Disorders
| Disorder | Typical Patient | Key Features | Diagnostic Clues | Management (1st-line / key) |
|---|---|---|---|---|
| PBC (Primary Biliary Cholangitis) | Middle-aged woman | Fatigue, pruritus, jaundice, xanthelasma | ↑ALP, +AMA (anti-mitochondrial antibody) | Ursodeoxycholic acid; transplant if end-stage |
| PSC (Primary Sclerosing Cholangitis) | Young/mid-aged man, IBD (esp. UC) | Fatigue, pruritus, jaundice | ↑ALP, p-ANCA; MRCP “beading” | Symptomatic Tx; stents; transplant definitive |
| Wilson’s Disease | Teen/young adult | Hepatitis/cirrhosis, neuro (tremor, dystonia, psych), Kayser–Fleischer rings | ↓Ceruloplasmin, ↑urinary copper | Chelation (penicillamine, trientine), zinc |
| Haemochromatosis | Middle-aged man | Bronze skin, diabetes, arthropathy, cirrhosis | ↑Ferritin, ↑TSAT; HFE mutation | Venesection (phlebotomy) |
| α-1 Antitrypsin Deficiency | Young adult | Cirrhosis + emphysema | ↓A1AT levels, PAS+ globules in hepatocytes | Supportive; transplant if severe |
 Management
Management
A) Acute Liver Failure (ALF)
What it is: sudden loss of hepatic function without prior cirrhosis; classic hallmark = INR (international normalised ratio) ≥1.5 + any encephalopathy.
Why dangerous: cerebral oedema, coagulopathy, sepsis → high short-term mortality
| Step | What to do |
|---|---|
| A–B–C | Airway (consider intubation if encephalopathy), Breathing, Circulation; escalate early to ICU/LTU (liver transplant unit). |
| N-acetylcysteine (NAC) | Give immediately in paracetamol ALF; consider in non-paracetamol ALF (benefit on transplant-free survival). |
| Monitor/replace | Hourly neuro obs; prevent hypoglycaemia (glucose infusion); correct K⁺/Mg²⁺/PO₄³⁻; manage coagulopathy only for procedures. |
| Infection | Culture blood/urine/ascites; treat sepsis early (broad-spectrum per local policy). |
| Avoid | Sedatives, unnecessary protein restriction, hepatotoxins; specialist management of raised ICP. |
| Transplant | Apply prognostic criteria (e.g., King’s concepts) and discuss listing early. |
B) Decompensated Cirrhosis
Why dangerous: each complication can rapidly precipitate multi-organ failure; always search for triggers (sepsis, GI bleed, alcohol/drugs, constipation, dehydration, electrolytes).
1) Ascites
What: pathological peritoneal fluid due to portal hypertension and sodium/water retention.
Why dangerous: SBP (spontaneous bacterial peritonitis), HRS-AKI (hepatorenal syndrome–acute kidney injury), malnutrition/respiratory compromise.
| Step | Treatment | Key notes |
|---|---|---|
| Initial | Alcohol stop; no NSAIDs; moderate salt restriction | Avoid very low protein diets. |
| Diuretics | Spironolactone up-titrate (e.g., 100 mg) ± furosemide (e.g., 40 mg) keeping 100:40 mg ratio | Target weight change 0.5 kg/day (no oedema) or 1 kg/day (with oedema). |
| LVP — Large-Volume Paracentesis | Remove >5 L ascites with albumin | Albumin ~8 g per L removed. |
| Refractory | Consider TIPS (transjugular intrahepatic portosystemic shunt) if suitable | Otherwise serial LVP + albumin. |
| Prophylaxis | Low ascitic protein (<15 g/L) or prior SBP → antibiotic prophylaxis | Follow local policy. |
2) SBP — Spontaneous Bacterial Peritonitis
What: infection of ascitic fluid without an obvious source.
Why dangerous: sepsis, renal failure, death if missed.
| Diagnosis | PMN ≥250/µL in ascitic fluid = treat now |
|---|---|
| Antibiotics | IV 3rd-gen cephalosporin (e.g., cefotaxime/ceftriaxone) then tailor to culture |
| Albumin | Day 1: 1.5 g/kg • Day 3: 1 g/kg (reduces renal failure/mortality) |
| Secondary prophylaxis | Long-term oral agent (e.g., quinolone) per local protocol |
3) Variceal Haemorrhage
What: bleeding from oesophageal/gastric varices due to portal hypertension.
Why dangerous: exsanguination, aspiration, encephalopathy.
| Immediate | Restrictive transfusion (Hb target ~70–80 g/L), terlipressin IV, prophylactic antibiotics (e.g., ceftriaxone) |
|---|---|
| Endoscopy | Urgent band ligation (EVL). If uncontrolled → balloon tamponade bridge; consider early TIPS in high-risk. |
| Secondary prevention | NSBB — Non-selective β-blocker (propranolol/carvedilol) + repeat EVL to eradication. |
| Primary prevention | For medium/large varices: NSBB or EVL if β-blocker contraindicated. |
4) Hepatic Encephalopathy (HE)
What: brain dysfunction from ammonia/toxins + precipitants (sepsis, bleed, constipation, electrolyte imbalance).
Why dangerous: airway risk, poor adherence, recurrent admissions.
| Precipitants | Sepsis, GI bleed, constipation, electrolyte imbalance, dehydration, sedatives |
|---|---|
| Treatment | Lactulose titrated to 2–3 soft stools/day; add rifaximin for recurrent HE or poor control; correct triggers; avoid sedatives |
5) HRS-AKI — Hepatorenal Syndrome (acute kidney injury)
What: functional renal failure in advanced cirrhosis due to extreme splanchnic vasodilation/renal vasoconstriction.
Why dangerous: rapid renal decline; mortality without reversal.
| Diagnosis | Cirrhosis + AKI not responding after diuretic stop and albumin 1 g/kg day 1 then day 2, with no shock/nephrotoxins/structural kidney disease |
|---|---|
| Treatment | Terlipressin + albumin; treat sepsis; consider TIPS in select cases; renal replacement as bridge; early transplant referral |
6) Hyponatraemia
What: dilutional fall in sodium from water retention (vasopressin excess) in cirrhosis.
Why dangerous: seizures if severe/rapid shifts; worsens encephalopathy.
| Principle | Fluid restrict if severe/symptomatic; stop offending drugs; slow correction (avoid osmotic demyelination). |
7) Nutrition
What: catabolic state with muscle loss and micronutrient deficiency.
Why dangerous: infections, falls, poor wound-healing, worse outcomes.
| Goals | 1.2–1.5 g/kg/day protein, frequent meals + late-evening snack; add vitamin D, zinc if low; no routine protein restriction once HE controlled; dietitian early. |
C) Chronic Cirrhosis — Clinic Bundle
What it is: long-term care to slow disease, prevent complications, and spot cancer early.
Why it matters: reduces admissions and mortality; identifies transplant candidates in time.
| Bundle | What to do |
|---|---|
| Aetiology therapy | Alcohol cessation; antivirals for HBV/HCV; immunosuppression for AIH; manage MASLD (weight, diabetes, lipids). |
| Varices | OGD screening; NSBB or EVL when indicated; educate re bleed signs. |
| Vaccines | HAV/HBV; influenza; pneumococcal as per local schedule. |
| HCC surveillance | Ultrasound ± AFP (alpha-fetoprotein) every 6 months for all cirrhosis. |
| Medicines review | Avoid NSAIDs; review ACEi/ARB/diuretics in AKI; PPI only if indicated (infection risk). |
| Transplant | Refer early if MELD-Na rising, refractory ascites, recurrent HE, recurrent variceal bleeding, or poor quality of life. |
| Supportive care | Frailty/bone health, falls prevention, nutrition, goals/ceilings of care discussion. |