
 Definition
Definition
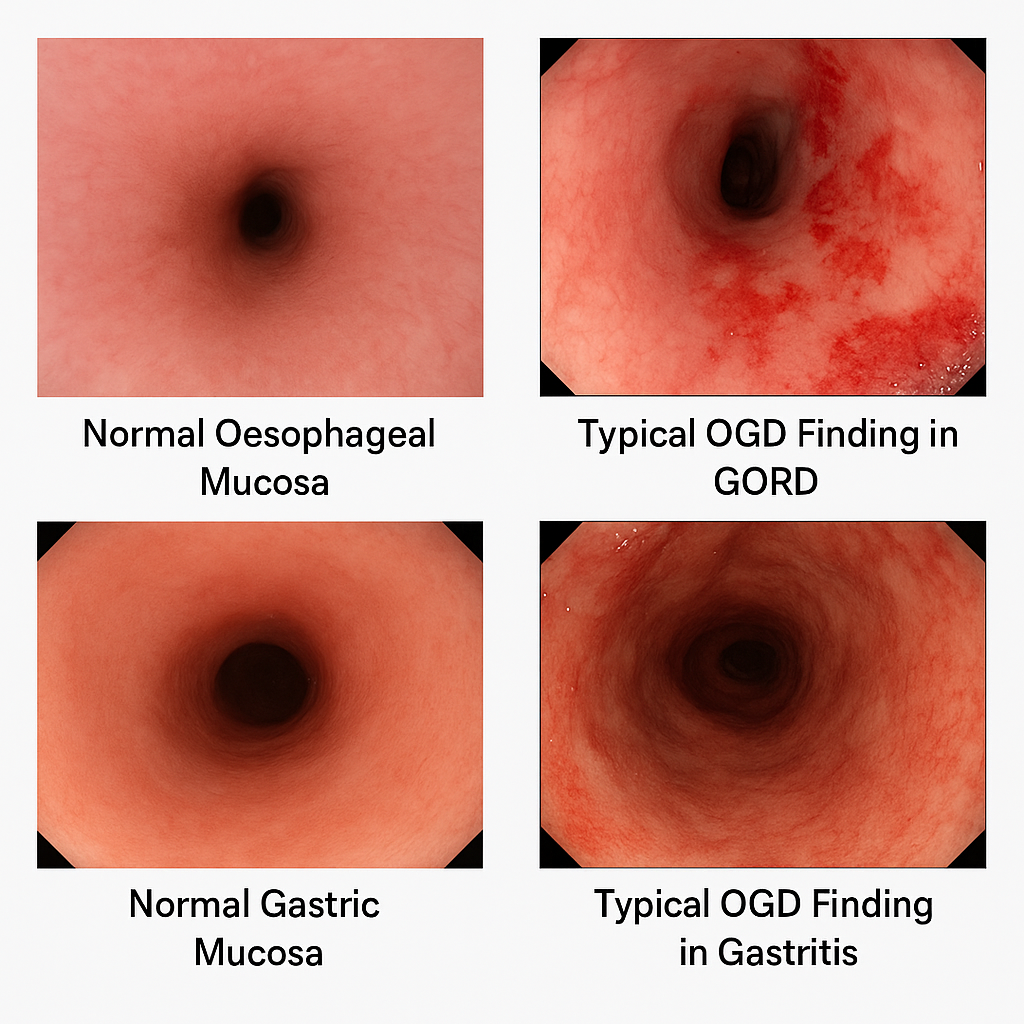
GORD: is a chronic condition where gastric acid refluxes into the oesophagus causing troublesome symptoms (e.g. heartburn) or complications (e.g. oesophagitis).
Gastritis: refers to inflammation of the gastric mucosa (acute or chronic) due to infection, irritants, autoimmune causes, or systemic disease.
 OGD Referral Criteria
OGD Referral Criteria
 Urgent — 2-Week Wait (ALARM55)
Urgent — 2-Week Wait (ALARM55)
Urgent referral for OGD (oesophagogastroduodenoscopy) (2WW) if:
- Anaemia (iron deficiency)
- Loss of weight (unintentional)
- Anorexia
- Recent onset dysphagia
- Melaena / haematemesis
- 55 years or older with new symptoms
2️⃣ Non-Urgent OGD — Barrett’s Risk Assessment
Consider non-urgent endoscopy for patients with GORD symptoms + multiple Barrett’s risk factors, even without red flags:
Chronic GORD symptoms (>5 years)
Age ≥50
Male sex
White ethnicity
Central obesity (waist circumference / BMI ↑)
Smoking history
First-degree relative with Barrett’s oesophagus or oesophageal adenocarcinoma
Purpose: Detect and confirm Barrett’s early for surveillance.
 Investigations
Investigations
| Test | Indication | Notes |
|---|---|---|
| Clinical diagnosis | Typical symptoms, no red flags | Empirical treatment appropriate |
| OGD | ≥55y + new symptoms • Alarm features • Poor treatment response | Biopsy if Barrett’s suspected |
| pH monitoring / manometry | Diagnosis uncertain after OGD | Useful for surgical planning |
| H. pylori testing | See treatment ladder | Stop PPI ≥2 weeks prior |
 Initial Assessment
Initial Assessment
Exclude red flags (↑ → urgent OGD)
Assess NSAID, alcohol, smoking use
Consider overlap with PUD or functional dyspepsia
 First-line in No Red Flags
First-line in No Red Flags
Lifestyle changes (see management)
Empirical PPI trial – omeprazole 20 mg OD for 4 weeks

 H. pylori Testing — When to Test?
H. pylori Testing — When to Test?
 Test for H. pylori if:
Test for H. pylori if:
- Un-investigated dyspepsia (especially <55 years and no red flags)
- Symptoms persist after PPI trial
- Previous history of gastric/duodenal ulcer or gastritis
- Planned long-term NSAID use, especially in patients >45 years
- Known iron-deficiency anaemia, or ITP/B12 deficiency
 Do not routinely test:
Do not routinely test:
Asymptomatic, no ulcer history or risk factors
During/within 2 weeks of PPI use
If alarm symptoms present → refer OGD
 PARA Tip:
PARA Tip:
PPIs must be stopped ≥2 weeks before urea breath test or stool antigen — common exam trap.

 H. pylori Testing — Which Test to Use?
H. pylori Testing — Which Test to Use?| Test | When to Use | Notes |
|---|---|---|
| Urea Breath Test | 1st-line | Stop PPI ≥2 wks before |
| Stool Antigen Test | 1st-line | Preferred in primary care |
| Serology | Avoid | Cannot distinguish past vs active infection |
| OGD + biopsy | Red flags / failure | Also rules out malignancy & ulcers |

 Follow-Up
Follow-Up
- Confirm eradication 4 weeks after completing triple therapy (if given) using urea breath test or stool antigen — not serology.
 Summary for PARA:
Summary for PARA:
Test H. pylori in persistent dyspepsia without alarm features. Use stool antigen or breath test (PPIs stopped 2 weeks prior). Do not test if alarm symptoms present — refer for endoscopy.
 Management —
Management —
Lifestyle & PRN Relief
Weight loss, smoking/alcohol cessation, avoid trigger foods/drinks, smaller frequent meals, avoid lying after eating, raise head of bed.
PRN antacids/alginates (e.g. Gaviscon Advance).
Standard PPI Trial
Omeprazole 20 mg OD × 4–8 weeks.
PHE advice: In uncomplicated dyspepsia, test for H. pylori after PPI trial (low UK prevalence <15%).
If improved → step down to lowest effective dose/on-demand.
Breakthrough Symptoms
Check adherence & lifestyle.
Offer PRN antacids between PPI doses.
If persistent → double PPI dose or trial alternative PPI.
Step-Up or Alternative
Double PPI dose (e.g. omeprazole 20 mg BD).
Switch to alternative PPI.
Add H2RA (e.g. famotidine) if PPI not tolerated.
H. pylori Eradication (if positive)
Triple therapy: PPI + amoxicillin + clarithromycin/metronidazole × 7 days.
Confirm eradication after 4 weeks (off PPI ≥2 weeks).
Refractory / Severe
OGD to rule out malignancy, Barrett’s, ulcers.
Consider surgical fundoplication for GORD if severe & PPI-resistant.
Manage autoimmune gastritis (lifelong B12 if pernicious anaemia).
 Complications
Complications
GORD – Mnemonic: BEACH
Barrett’s oesophagus
Esophagitis
Anaemia
Carcinoma (adenocarcinoma risk)
Haematemesis
Gastritis – Mnemonic: BAGS
- Bleeding
- Anaemia
- Gastric atrophy
- Stomach cancer